Introduction
Physical therapy in Catonsville and Sykesville for Pediatric Issues
Welcome to Catonsville and Sykesville Physical Therapy’s resource about slipped capital femoral epiphysis.
Slipped capital femoral epiphysis (SCFE) is a condition that affects the hip in teenagers between the ages of 12 and 16 most often. Cases have been reported as early as age nine years old. In this condition, the growth center of the hip (the capital femoral epiphysis) actually slips backwards on the top of the femur (the thighbone). If untreated, this can lead to serious problems in the hip joint later in life. Fortunately, the condition can be treated and the complications avoided or reduced if recognized early.
Surgery is usually necessary to stabilize the hip and prevent the situation from getting worse.
This guide will help you understand:
- what can cause this condition
- what the symptoms are
- how your health care professional will diagnose the condition
- what treatment options are available
- what Catonsville and Sykesville Physical Therapy’s approach to rehabilitation is
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Pediatrics|limit:15|heading:Hear from some of our *Pediatrics* patients#
Anatomy
What part of the hip is affected?
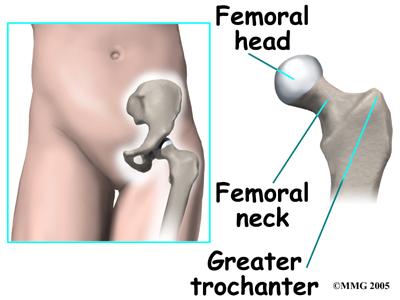
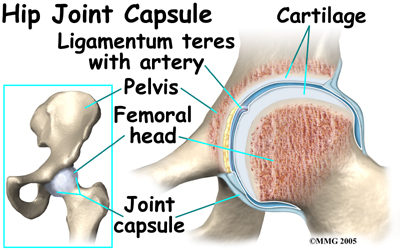
The hip joint is where the thighbone (femur) connects to the pelvis. The joint is made up of two parts. The upper end of the femur is shaped like a ball. It is called the . The femoral head fits into a socket in the pelvis called the acetabulum. This ball-and-socket joint is what allows us to move our leg in many directions in relation to our body.
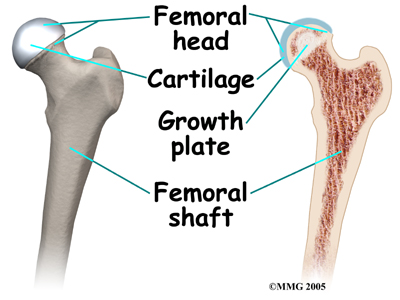
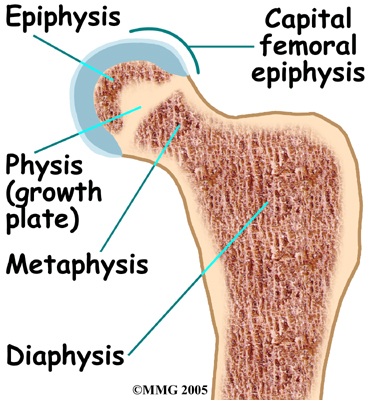
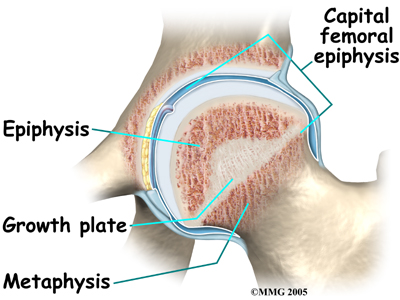
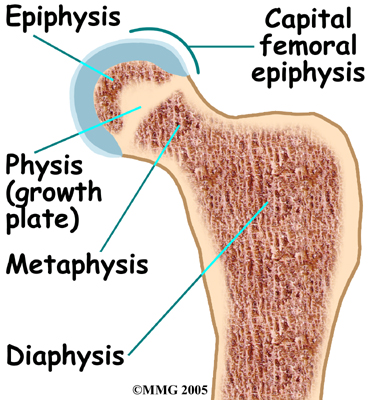
In the growing child, there are special structures at the end of most bones called growth plates. The growth plate is sandwiched between two special areas of the bone called the epiphysis and the metaphysis. The growth plate is made of a special type of cartilage that builds bone on top of the end of the metaphysis and lengthens the bone as we grow. In the hip joint, the femoral head is one of the epiphyses of the femur. The capital femoral epiphysis is somewhat unique. It is one of the few epiphyses in the body that is inside the joint capsule. (The joint capsule is the tissue that surrounds the joint.)
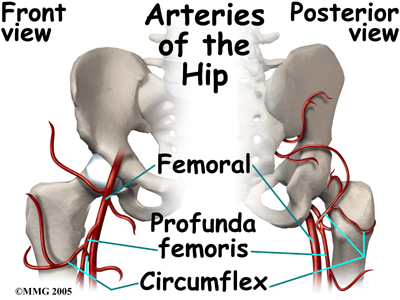
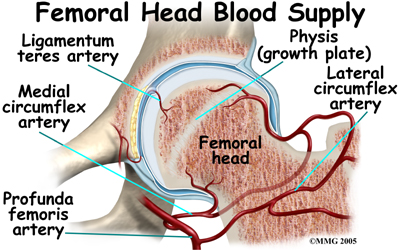
The blood vessels that go to the epiphysis run along the side of the femoral neck and are in danger of being torn or pinched off if something happens to the growth plate. This can result in a loss of the blood supply to the epiphysis.
Causes
How does this problem develop?
SCFE develops at a specific age. The changes occurring in the growing skeleton during puberty play into the chances that a child will develop SCFE. The cartilage epiphyseal plate is weaker than the surrounding bone. Children who are overweight are more prone to developing SCFE. This suggests that the main cause of SCFE is from increased force on the hip at a time when the femoral head is not quite ready to support these forces. The femoral head fails at the weakest point, through the epiphyseal plate. As a result, a condition similar to a stress fracture develops.

SCFE may affect both hips. In fact, 20 to 40 percent of the time the condition is bilateral (meaning that it affects both hips). Only one hip may be painful, so it is common for doctors to carefully watch the other hip to recognize the disease as early as possible. The earlier the diagnosis is made, the more effective the treatment. Studies have shown that the more severe the slip, the worse the long-term outcomes. The earlier the diagnosis is made, the more effective the treatment.
Symptoms
What does the problem feel like?

Most teenagers with SCFE develop pain in the hip, and they begin to walk with a limp. In addition, the motion of the hip is abnormal and restricted. Because the anatomy of the hip joint is altered, patients usually walk with the foot and leg turned out on the affected side.
Interestingly, problems in the hip sometimes do not cause pain in the hip itself. The knee is where the pain is felt. This can be confusing both to patients and health care professionals. In general, a teenager with knee pain who has no clear-cut reason to have knee pain should be examined for possible SCFE. This usually includes X-rays of the hips to make sure that SCFE is not missed.
 The main problem with SCFE is that it changes the structure of the hip joint. How much it affects the way the hip joint works depends on how much the epiphysis slips. The more the slip, the more likely there will be problems later in life.
The main problem with SCFE is that it changes the structure of the hip joint. How much it affects the way the hip joint works depends on how much the epiphysis slips. The more the slip, the more likely there will be problems later in life.
In general, the most common problem later in life is the development of arthritis in the hip joint. The type of arthritis that develops in the hip is osteoarthritis (also known as wear-and-tear arthritis). Just like a machine that is out of balance, the hip joint wears out and becomes painful.
There are two complications of SCFE that may occur immediately after the condition develops. The first complication is , a condition where the articular cartilage of the hip joint is destroyed. Articular cartilage is the smooth material that covers the joint surface. It is unclear why this condition develops. It may occur if the SCFE has been treated with or without surgery. This condition results in narrowing of the joint space and a painful, stiff hip.
The other possible complication is called of the capital femoral epiphysis. This usually occurs when the blood vessels that provide blood to the epiphysis are damaged, torn, or pinched. This can happen when the SCFE develops very rapidly and presents like a true fracture. This can also occur when attempting to reduce, or align, the two parts of the femoral head before inserting a screw. The result is that the epiphysis dies and the bone collapses causing further deformity. This can lead to early arthritis in the hip joint.
Diagnosis
How do health care professionals identify the problem?
At Catonsville and Sykesville Physical Therapy your physical therapist will initially take a thorough history of when and how your child’s pain started. It is important to for us to determine if the pain began insidiously (for no particular reason) or occurred as a result of a trauma (i.e.: a fall or specific incident.) SCFE pain is generally of insidious onset. In deducing the cause of the pain it is also important for us to determine if the pain is constant or occurs only with specific activities. Pain caused by SCFE is more likely to be relatively constant but can increase during weight bearing activities. If your child is walking with a limp or with an altered foot position due to the pain, your physical therapist may ask to watch your child walk to assess the limp during the gait cycle.
Next your Catonsville and Sykesville Physical Therapy physical therapist will then palpate around any areas of pain. . As mentioned above, the pain from SCFE is most often felt in the hip but may also cause pain in the knee. For this reason we may also palpate around the knee. We may also need to examine related areas such as the low back or anywhere along the lower limb in order to identify the location of the actual problem.
Following palpation your physical therapist will assess the range of motion of your child’s joints and compare them to the other side. They will also check the strength of the muscles on both sides and may check for the integrity of the ligaments around the joints.
The history, and physical examination are usually enough to make a health care professional highly suspicious about the diagnosis of SCFE in children of the appropriate age. If SCFE is suspected, your Catonsville and Sykesville Physical Therapy physical therapist will recommend that your child is reviewed by a doctor for investigative tests to confirm or rule out this diagnosis.
Catonsville and Sykesville Physical Therapy provides services for physical therapy in Catonsville and Sykesville.
Our Treatment
What treatment options are available?
Nonsurgical Treatment
Treatment of SCFE usually requires surgery. If surgery is absolutely not possible for other reasons, then placing the child in a type of body cast called a hip spica may be an option. This is not as successful as surgery and is not the preferred choice.
Surgery
The primary goal of the treatment of SCFE is to stop any further slippage of the capital femoral epiphysis. The less slip, the lower the risk of problems in the hip during the child's life.
Once the epiphysis has closed, slippage will stop. Epiphysis closure occurs when the two areas of bone, the epiphysis and metaphysis, join, or fuse, into one single bone. At that point there is no cartilage growth plate remaining between the two parts of the femur. Surgery usually speeds up the process of epiphysis closure.
 Once the diagnosis of SCFE is made, surgery is usually recommended immediately. The surgery is scheduled within a few days following the diagnosis. Until the surgery can be performed, it is highly advisable to use crutches and restrict activities to a minimum in order to decrease pain and stop any further slippage. The surgery can usually be done as an outpatient. General anesthesia (where the patient is put completely to sleep) is usually recommended, unless there are reasons not to use a general anesthetic. If so, a spinal block may be used instead.
Once the diagnosis of SCFE is made, surgery is usually recommended immediately. The surgery is scheduled within a few days following the diagnosis. Until the surgery can be performed, it is highly advisable to use crutches and restrict activities to a minimum in order to decrease pain and stop any further slippage. The surgery can usually be done as an outpatient. General anesthesia (where the patient is put completely to sleep) is usually recommended, unless there are reasons not to use a general anesthetic. If so, a spinal block may be used instead.
The preferred method for stopping the epiphysis from slipping further is to into the epiphysis to hold it in place. This screw is placed using a special X-ray machine called a fluoroscope. The fluoroscope allows the surgeon to see an X-ray image on a TV monitor while doing the surgery. In this way, the surgeon is able to accurately place a screw into the epiphysis using a small incision in the side of the thigh.
Other types of surgery have been used in the past. For many years surgeons thought it necessary to use two or three screws to hold the epiphysis. This has been shown to be unnecessary in most cases. Using additional screws may actually increase the risk of complications. Open operations using much larger incisions have also been used in the past. These procedures have been abandoned because using a single screw works better and is easier to do.
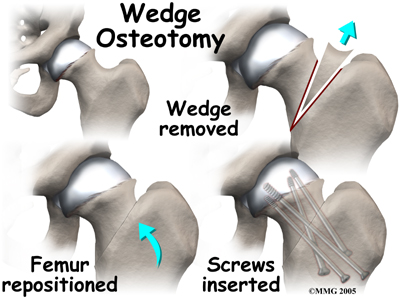
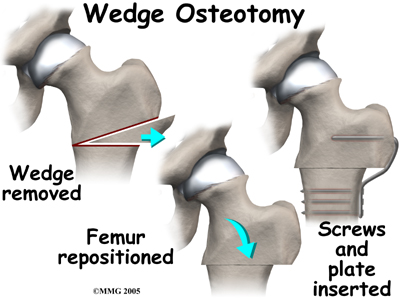
If there is a serious structural change in the anatomy of the hip, there may need to be further surgery to restore the alignment closer to normal. This procedure is usually not considered until the child is done growing. As a child grows, there will be some remodeling that occurs in the hip joint. This may improve the situation such that further surgery is unnecessary.
In the case of unilateral (one-sided) SCFE, experts also recommend pinning the normal hip. This is called prophylactic pinning. The child with moderate to severe unilateral SCFE is at risk for slippage to occur on the other side.
Prophylactic treatment is easy to do and can be done at the time of the operation on the involved side. Taking this step reduces the need for repeated X-rays to check the normal side for any sign of SCFE. The child can remain more active without constant worry that the hip will slip. The complications of chondrolysis, avascular necrosis, and/or degenerative arthritis can also be avoided.
Post surgically the surgeon will take X-rays to make sure that the screw remains in the right place. The X-rays are also required to determine when the epiphyseal plate fuses. At that point, there won't be any chance that the slip will get worse. When it is confirmed that the plate has fused, the follow up visits will be focused on whether the abnormality is likely to need any additional surgery to realign the hip.
Opinions differ on the need to remove the screw once the epiphysis has fused. Removing the screw requires a second surgery that can be expensive and carries a slight risk due to the need for anesthesia. The hole left when the screw is removed also increases the risk of fracture after the screw is taken out. If the screw is removed, the surgeon may recommend crutches for three to six weeks afterward. Many surgeons feel that the screw should be left in place if it isn't causing problems.
Rehabilitation
What should be expected from rehabilitation post surgery?
Following surgery for SCFE, physical therapy treatment is very useful in returning your child to their pre-injury activity level as quickly as possible. Physical therapy can also assist in avoiding other compensatory problems in the back or lower limb in the future. Catonsville and Sykesville Physical Therapy provides services for physical therapy in Catonsville and Sykesville.
Rehabilitation at Catonsville and Sykesville Physical Therapy can begin as soon as your child’s surgeon recommends it. Each surgeon will set his or her own specific restrictions based on the child’s individual severity of injury, the surgical procedure used, personal experience, and whether the SCFE is healing as expected.
Initially your physical therapist at Catonsville and Sykesville Physical Therapy may use modalities such as heat, ice, ultrasound, or electrical current to assist with decreasing any pain associated with the surgery. Crutches and a non-weight bearing status are standard following surgery for SCFE but within three to five days most patients will be able to start putting some weight down while standing or walking. Your physical therapist at Catonsville and Sykesville Physical Therapy will ensure your child is using the crutches safely and appropriately and that they are abiding by the weight bearing restrictions set by their surgeon. Your physical therapist will also ensure that your child can safely use the crutches on stairs. We generally recommend that until it is possible to walk without a significant limp, either one or two crutches continue to be used. Improper gait can lead to a host of other pains in the knee; hip and back so it is prudent to continue on crutches until near normal walking can be achieved. Your Physical therapist will give advice regarding the appropriate time for your child to be walking without any support at all. Once the crutches are no longer required, your physical therapist will assist with gait re-education.
The next part of our treatment at Catonsville and Sykesville Physical Therapy will focus on normalizing any deficits that may have developed in the range of motion and strength of your child’s lower limb joints. Your physical therapist may assist in stretching your child’s limb or lower back while at the clinic and, if necessary, will ‘mobilize’ the joints of your child. This hands-on technique encourages the stiff joints to move gradually into their normal range of motion. In addition to the hands-on treatment in the clinic we will also prescribe a series of stretching exercises that we will encourage your child to do as part of a regular home exercise program.
Similarly to the range of motion deficits, strength deficits will also be addressed. Strength building exercises will be taught in the clinic and added to their home program. We may incorporate items such as Theraband or light weights into the exercises to provide additional resistance for the limb.
The final part of our Catonsville and Sykesville Physical Therapy treatment will be ensuring that your child’s coordination and balance have returned to normal after their surgery. Following even a short period of walking with crutches or with an altered weight bearing status, your child’s normal balance, coordination, and proprioception (the ability to know where your body is without looking at it) can decline in function. Exercises, which may include balancing on one foot, jumping, and quick agility movements will be encouraged at an appropriate time in line with the surgeon’s restrictions.
Fortunately, gaining lost range of motion, strength, and coordination after surgery for SCFE goes quickly. You will notice improvements in your child’s function and gait even after just a few treatments with your physical therapist at Catonsville and Sykesville Physical Therapy. If, however, your child’s post-surgical physical therapy is not progressing as your physical therapist would expect, we will ask you to follow-up with your surgeon to confirm that the hip is tolerating the rehabilitation well and ensure that there are no post-surgical complications that may be impeding your child’s recovery.
Catonsville and Sykesville Physical Therapy provides services for physical therapy in Catonsville and Sykesville.
Portions of this document copyright MMG, LLC









